Bespoke Architecture and Longevity
The question of how long a person lives has been studied primarily through the lens of medicine and genetics. Architecture rarely enters that conversation. This research proposes that it should — not as a peripheral variable but as a primary environmental condition that shapes the physiological and psychological systems governing both the quality and duration of human life.

Is longevity determined by genetics?
Genetics establishes predispositions — inherited tendencies toward certain diseases, metabolic patterns, and baseline physiological capacities. But the genetic argument for longevity is incomplete without its environmental counterpart. Access to clean air and water, the quality of housing, the safety of the surrounding urban fabric, and the availability of medical infrastructure all operate alongside genetic inheritance to determine how long and how well a person lives. The twentieth century’s dramatic increase in average human lifespan was not primarily a genetic event. It was an environmental and infrastructural one. This distinction is the foundation of this research: if environment shapes lifespan as powerfully as genetics, then the design of that environment is a medical question as much as an architectural one.
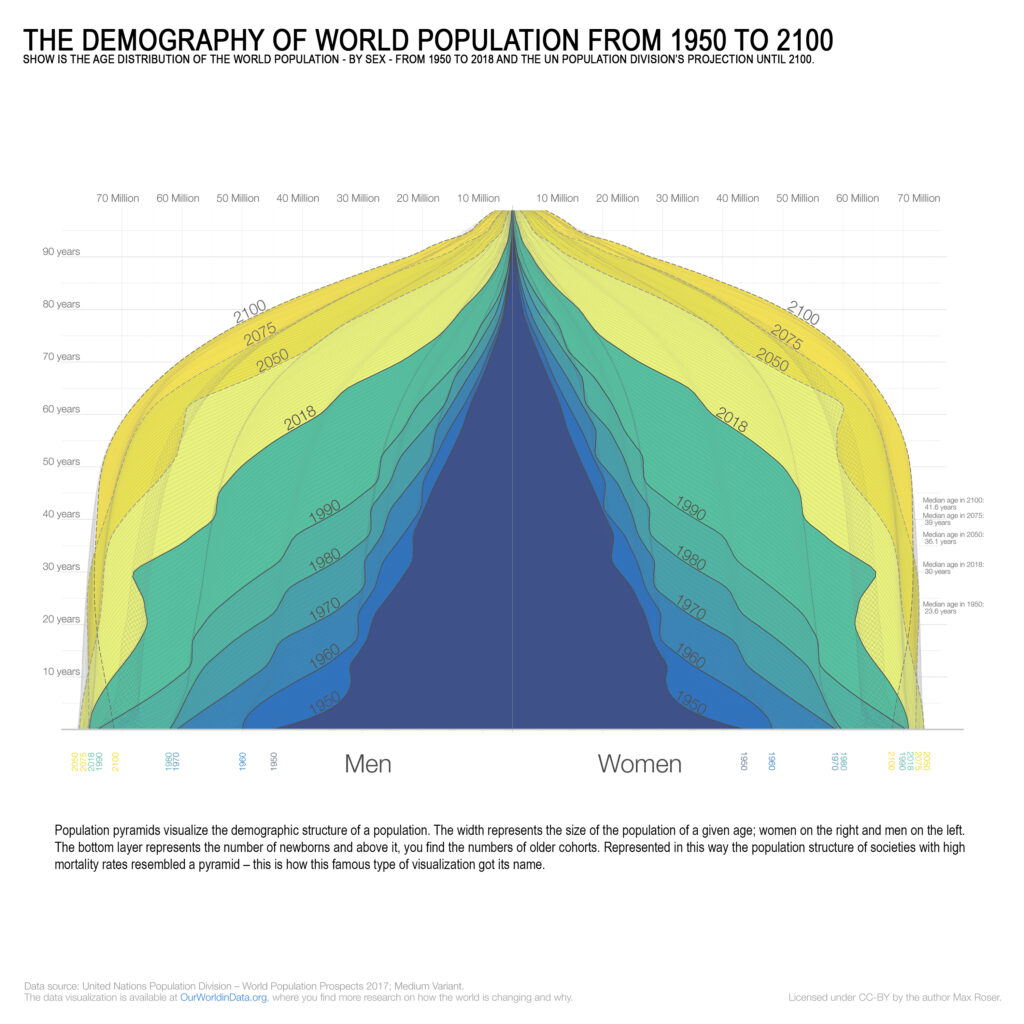
The Demography of the World Population from 1950 to 2100
Population pyramids record the consequence of this relationship between environment and lifespan over time. Their shape is not fixed — it changes as the conditions governing mortality change. Societies with high mortality rates produce true pyramids: wide bases of young people tapering sharply toward older age groups. As environmental quality improves — through better housing, cleaner water, more walkable cities, access to natural light — the pyramid’s upper sections widen. The graphic record of global demographic change from 1950 to 2100 shows this transformation in progress: a world in which the traditional pyramid is gradually replaced by a column, the older age groups filling in as the conditions that previously eliminated them are addressed. Architecture is among the conditions being addressed.
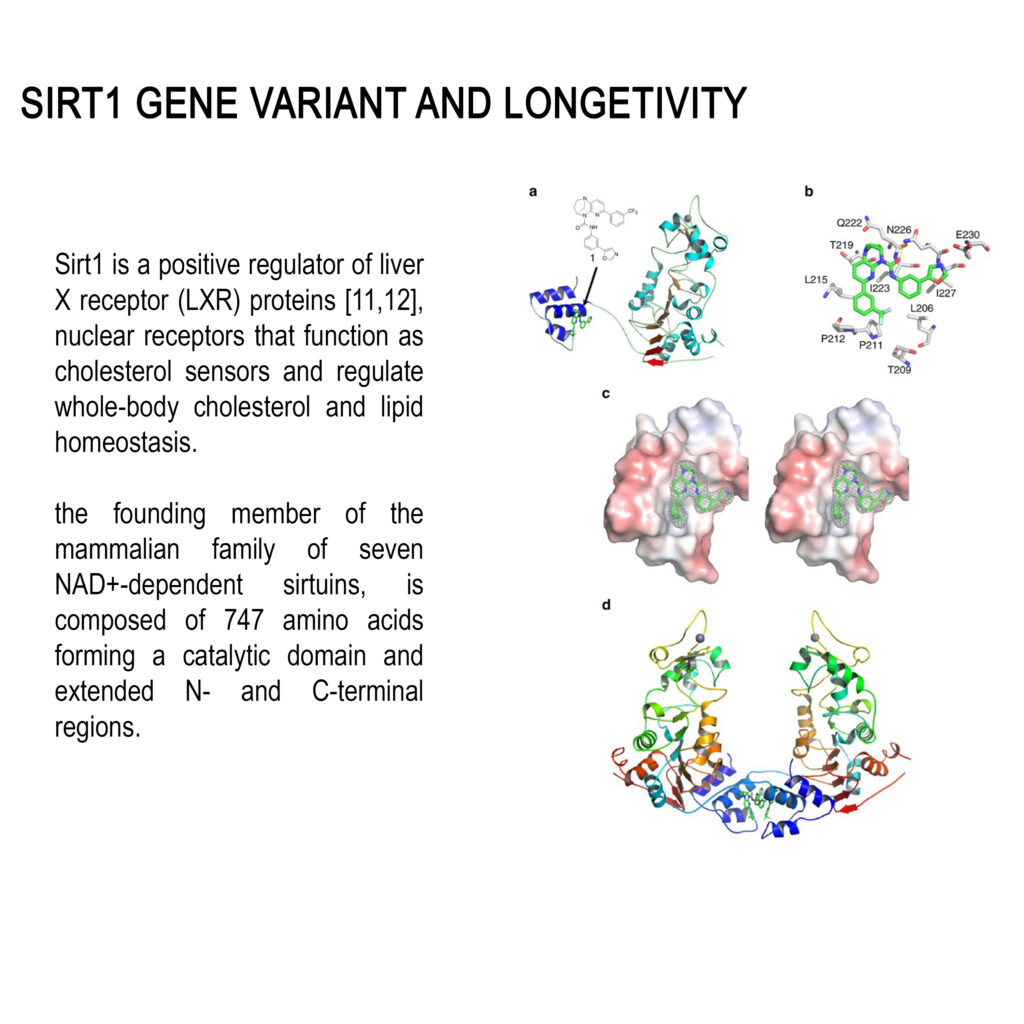
Sirt1 Gene Variant and Longevity
At the molecular scale, the Sirt1 gene variant provides a biological reference point for understanding how environment and longevity intersect at the cellular level. Sirt1 is a positive regulator of liver x receptor proteins — nuclear receptors that function as cholesterol sensors and govern whole-body cholesterol and lipid homeostasis. As the founding member of the mammalian sirtuin family, it is composed of 747 amino acids forming a catalytic domain with extended terminal regions. Its activity is responsive to environmental inputs including caloric availability, stress exposure, and sleep quality — the same conditions that architectural design directly influences. A building that improves sleep, reduces stress, and supports physical activity is, at the molecular level, a building that supports the conditions under which Sirt1 operates most effectively.
Air, sleep, and movement
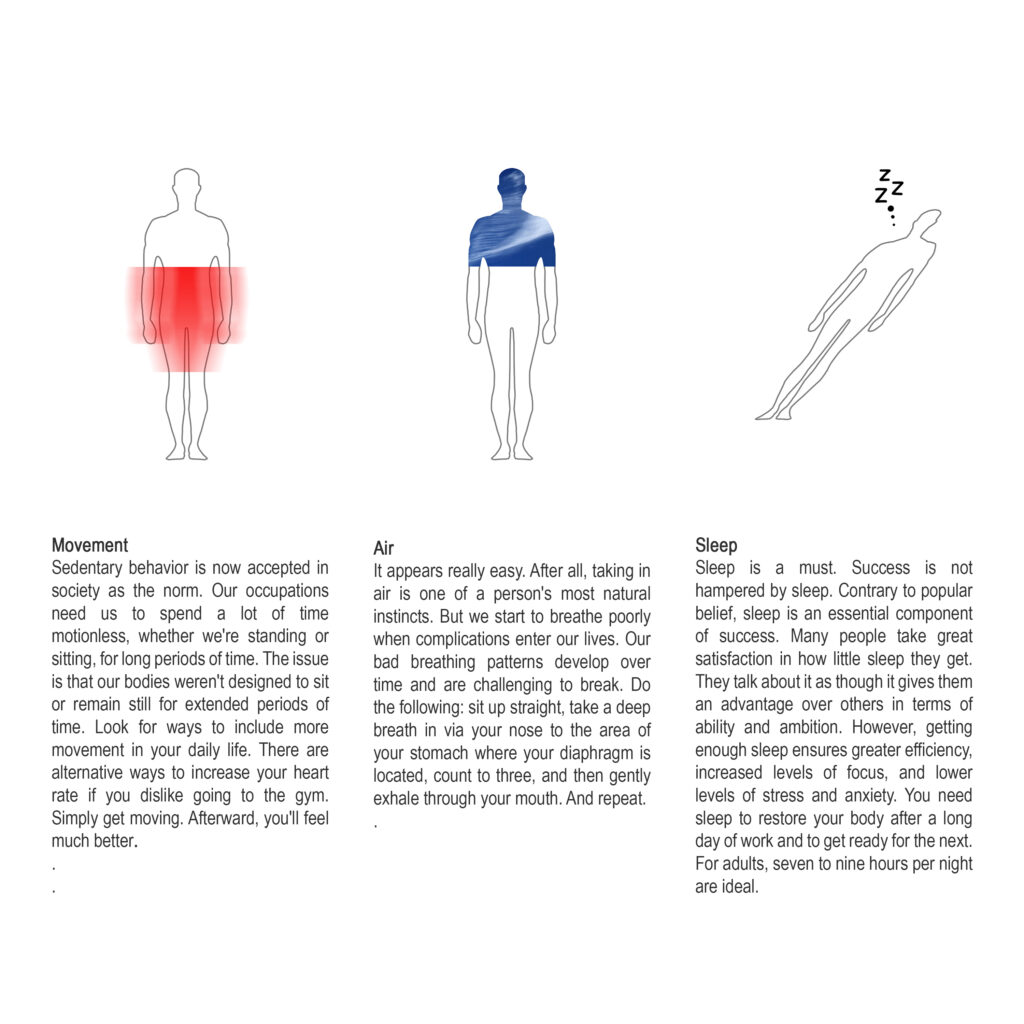
Three physiological inputs — air quality, sleep quality, and physical movement — collectively form the baseline of a longer and healthier life. Each is directly shaped by architectural and urban decisions. Air quality inside a building is a function of its ventilation strategy, its material specification, and its relationship to the outdoor environment. A building with poor air circulation, off-gassing synthetic materials, and no connection to natural airflow degrades the respiratory and cardiovascular health of its occupants regardless of how medically attentive those occupants are. Sleep quality is governed by acoustic performance, light control, and thermal comfort — all design variables. A bedroom that admits excessive noise, fails to block artificial light, or fluctuates in temperature across the night produces poor sleep, and poor sleep produces measurable consequences: weakened immune function, cognitive decline, elevated risk of diabetes, obesity, and cardiovascular disease. Physical movement is encouraged or discouraged by spatial layout. A building whose circulation routes are interesting, whose stairs are visible and accessible, and whose relationship to the surrounding landscape invites walking produces more physical activity in its occupants than one that routes everyone to an elevator and deposits them at a parking structure. These are not incidental design outcomes — they are the direct physiological consequences of architectural decisions made at the drawing stage.
A person’s need to live better
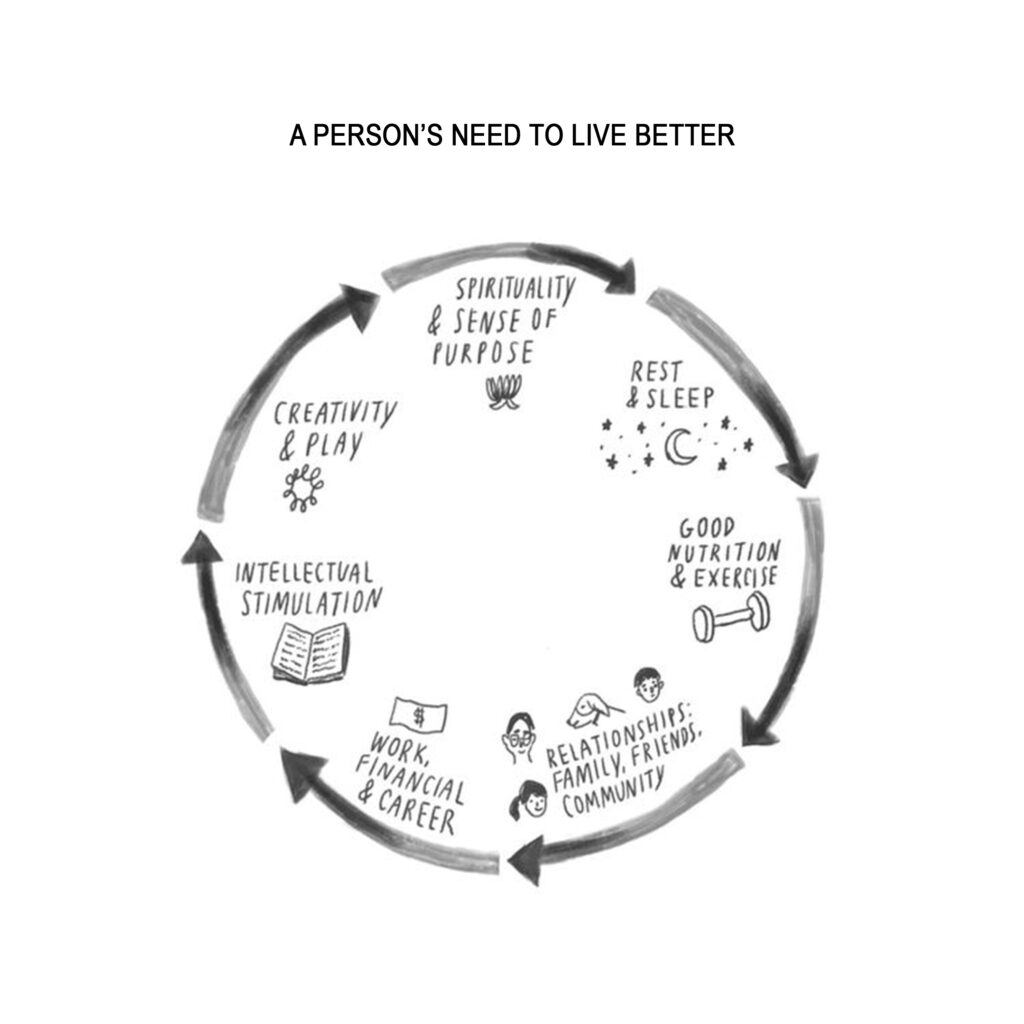
The conditions that support a better life extend beyond the purely physical. Spirituality and a sense of purpose, restorative rest, meaningful relationships, intellectual stimulation, creative expression, and financial stability all contribute to the psychological and social dimensions of longevity. Architecture addresses each of these not by providing them directly but by creating the spatial conditions under which they become possible. A home with a space for quiet contemplation supports the development of spiritual practice. A neighborhood designed for chance social encounters supports the maintenance of community relationships. A workplace that provides natural light and varied spatial experiences supports cognitive performance. A city that integrates green space, mixed-use proximity, and walkable infrastructure supports the daily physical and social habits that collectively extend life. The building is not a neutral container for these activities — it is an active participant in whether they occur.
Architecture and sports and health
The integration of architectural design with the conditions for physical activity operates across multiple scales simultaneously. At the building scale, the placement of stairs, the presence of courtyards, and the connection to outdoor space all influence how much a resident moves through the course of a normal day. At the neighborhood scale, the proximity of parks, cycling infrastructure, and pedestrian routes determines whether physical activity requires a deliberate effort or happens naturally as a byproduct of daily life. At the urban scale, the distribution of recreational facilities, the safety and quality of public space, and the inclusivity of design for different ages and physical capacities establish whether a city’s population maintains physical health across its full lifespan or concentrates that health in the demographic that can afford private gyms. Nature-integrated settings — courtyards with planting, terraces overlooking green ground, facades that admit natural light and air — reduce the stress hormones that suppress immune function and increase the regenerative conditions under which the body repairs itself. These are not arguments for aesthetics. They are arguments for the biological consequences of spatial design.
Urban planning and the quality and length of life
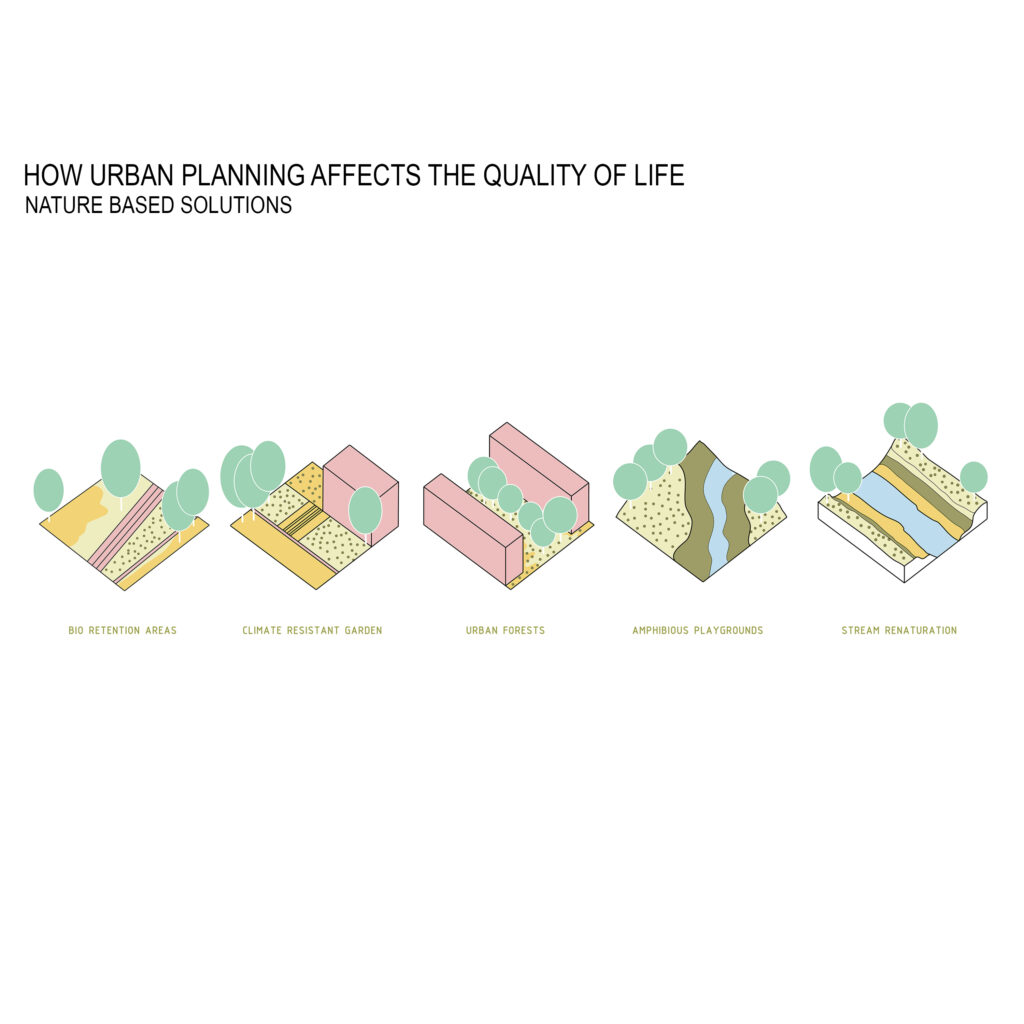
Urban planning operates at the scale where individual architectural decisions accumulate into systemic health outcomes. The distribution of green space across a city determines the average distance a resident must travel to access nature — and research consistently shows that proximity to green space reduces stress, encourages physical activity, and improves mental health outcomes across the full population. The provision of pedestrian and cycling infrastructure determines how much incidental physical activity is built into daily commuting. The proximity of healthcare facilities determines how quickly acute health events are addressed before they become chronic conditions. The integration of fresh food retail into residential neighborhoods determines dietary quality. The control of industrial and traffic pollution determines respiratory health across the city’s lifetime. None of these are luxury provisions — they are the baseline conditions of urban health, and their quality is determined by planning decisions made decades before their consequences become visible in mortality statistics. The city that invests in these conditions at the planning stage is investing in the longevity of its population. The city that defers them is deferring a health cost that will be paid by its hospitals.

Architecture: need or luxury?


The framing of architecture as either necessity or luxury is a false binary. A building that provides ergonomic comfort, efficient spatial organization, spaces for quiet contemplation, and environments that support self-awareness is not luxurious in the sense of excess — it is precisely calibrated to the conditions under which human beings function at their most effective. Ergonomics reduces the physical stress that accumulates in poorly designed workplaces and living environments, producing long-term musculoskeletal and cardiovascular consequences. Spatial clarity reduces the low-level cognitive load that accompanies navigating confusing or poorly organized environments, a load that contributes cumulatively to stress and mental fatigue. Spaces that invite contemplation — a window that frames a view, a corner that offers quiet within a larger open plan, a transition between spaces that creates a moment of pause — support the psychological recovery that a continuously stimulated mind requires. These are not amenities. They are the spatial equivalents of sleep and exercise: conditions that the body and mind require to function and that architecture either provides or withholds.
Urban interventions and effects

Urban interventions that succeed share five qualities: they are lively, healthy, attractive, sustainable, and safe. These are not independent criteria — they are mutually reinforcing conditions. A public space that is perceived as unsafe will not be used, and a space that is not used will not be lively, and a space that is not lively will not attract the social interaction that produces community health. The sequence runs in reverse as well: a space that is beautifully designed invites use, use produces social encounter, social encounter generates the sense of safety that comes from eyes on the street, and safety sustains the continued investment in the space’s quality. Urban interventions that understand this interdependence produce spaces that become self-sustaining civic assets. Those that address only one criterion — safety without attractiveness, or attractiveness without vitality — produce spaces that are used briefly and abandoned. The measure of a successful urban intervention is not how it looks at opening but how it is used ten years later.
Colors and quality and length of life

Color is not a finishing decision — it is an environmental condition with measurable physiological and psychological consequences. Warm hues in the red and orange range activate and energize; they are appropriate for spaces designed for physical activity and social engagement. Cool tones in the blue and green range reduce heart rate and cortisol levels; they are appropriate for spaces designed for rest and recovery. Light tones expand the perceived volume of a space, reducing the sense of compression that produces low-level stress in confined environments. The chromatic relationship between a space and its cultural context determines whether its occupants feel located or displaced — a dimension of color that matters particularly in cultures with strong visual traditions. The cumulative effect of inhabiting color environments that are inappropriate to their function is a chronic, low-level stress that contributes to the same physiological degradation as poor air quality or poor sleep. Color is not decoration applied after the architecture is resolved. It is part of the architecture’s environmental performance specification.
How does the quality of materials affect us

Material quality in architecture operates at two levels: the chemical and the haptic. At the chemical level, synthetic materials that off-gas volatile organic compounds degrade indoor air quality continuously over the lifetime of the building, producing respiratory and neurological consequences in their occupants that accumulate over years of exposure. Natural materials — stone, wood, unfinished metals — do not carry this liability, and their thermal mass properties contribute to the stable internal temperature conditions that support sleep quality and metabolic function. At the haptic level, the tactile quality of surfaces that are touched daily — door handles, handrails, flooring, countertops — contributes to the sensory experience of inhabitation in ways that synthetic substitutes do not replicate. The neurological engagement of touching a material that has depth and variation is measurably different from touching one that is uniform and inert. This is not sentimentality. It is the architecture of sensory engagement, and sensory engagement is a component of psychological health. The emergence of digital fabrication technologies including three-dimensional printing extends the range of material geometries available for architectural application, making it possible to specify complex surface conditions at production cost. The question this raises for architecture is not what can be made but what should be made — which material conditions best serve the physiological and psychological health of the people who will inhabit the result.
The emotional dimension of architecture is inseparable from its capacity to establish a sense of place. A building that produces a coherent and distinctive spatial identity — through the consistency of its material palette, the clarity of its organizational logic, the quality of its relationship to light and landscape — generates the feeling of belonging that supports psychological stability. Belonging is not a luxury experience. It is a measurable component of mental health, and its absence contributes to the anxiety and social disconnection that degrade both quality and length of life. A building that produces no sense of place, that could be anywhere and therefore is nowhere, deprives its occupants of one of the fundamental psychological resources that architecture is positioned to provide.
Altitude provides an instructive natural experiment in the relationship between environment and cardiovascular health. Populations living at elevation adapt to reduced oxygen availability through measurable improvements in cardiovascular efficiency — enhanced heart capacity and the potential for extended lifespan among them. The mechanism is environmental stress producing physiological adaptation. Architecture cannot replicate altitude, but it can replicate the conditions that altitude produces: spaces that require physical exertion as a normal part of daily life, that provide clean air, that connect inhabitants to natural conditions rather than insulating them from all environmental variation. The completely climate-controlled, mechanically sealed building that admits no variation of light, air, or temperature across the day or across the year is not a health environment — it is a sensory deprivation environment in which the body’s adaptive mechanisms have nothing to adapt to.

Research into quality of life has historically focused on three dimensions: physical health, psychological well-being, and social functioning. Recent scholarship has identified the environment as a fourth dimension of comparable significance — not a backdrop to the other three but an active determinant of them. The environment shapes physical health through air quality, thermal comfort, and the conditions for movement. It shapes psychological well-being through spatial clarity, sensory richness, and the provision of restorative spaces. It shapes social functioning through the design of shared spaces, the management of acoustic conditions that allow conversation, and the spatial organization of neighborhoods that makes social encounter a natural byproduct of daily movement. Architecture is the discipline that designs the environment. The implication is that architects are health practitioners operating at the scale of cities.

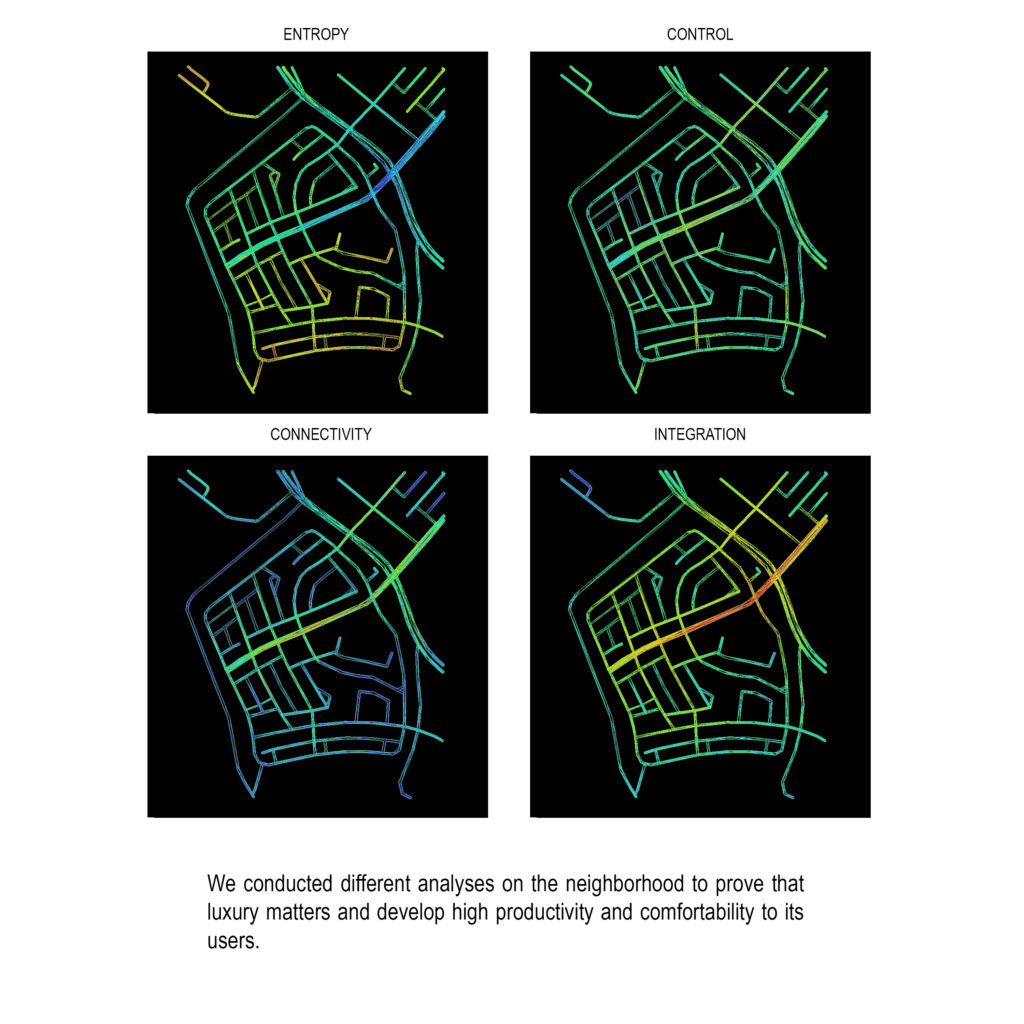
The neighborhood of Dhahran in the Eastern Province of Saudi Arabia provides a concrete illustration of the relationship between environmental quality and economic productivity. With a GDP per capita of $55,940 — the highest in the Middle East after Qatar — Dhahran demonstrates that the investment in high-quality built environment is not a cost that economically productive communities bear but a condition that economically productive communities require. The correlation between the quality of the spatial environment and the productivity of its inhabitants is not coincidental. It reflects the direct relationship between the physiological and psychological conditions that good architecture provides and the cognitive and physical performance that those conditions support.






Conclusion
The evidence assembled in this research points consistently toward a single conclusion: architecture is not neutral with respect to human health and longevity. The spatial conditions in which people sleep, move, breathe, work, and recover from the demands of daily life are not incidental to the outcomes of those activities. They are constitutive of them. A building that admits natural light, circulates clean air, specifies non-toxic materials, provides spaces for both social engagement and quiet recovery, and connects its occupants to the natural landscape is a building that supports longer and better lives. This is not a description of luxury architecture in the sense of excess or indulgence. It is a description of architecture that takes its health obligations seriously — that understands the design of the built environment as an act with consequences for the biological systems of the people who inhabit it. The relationship between the quality of architectural design and the quality of human life is not aspirational. It is measurable, documented, and waiting to be designed for.
The design principles that govern this approach at INJ Architects are developed further in how-we-work. For clients seeking residential or institutional commissions where the health performance of the built environment is treated as a primary design brief, the engagement framework is outlined in bespoke-architecture.
“`